Chinese Journal of Tissue Engineering Research ›› 2014, Vol. 18 ›› Issue (31): 5062-5067.doi: 10.3969/j.issn.2095-4344.2014.31.024
Previous Articles Next Articles
Evaluation for fracture risk in elderly patients after hemiarthroplasty
Hua Han-bing, Bi Zheng-gang
- Department of Orthopedic Surgery, First Affiliated Hospital, Harbin Medical University, Harbin 150001, Heilongjiang Province, China
-
Received:2014-06-10Online:2014-07-23Published:2014-07-23 -
About author:Hua Han-bing, Studying for master’s degree, Physician, Department of Orthopedic Surgery, First Affiliated Hospital, Harbin Medical University, Harbin 150001, Heilongjiang Province, China
CLC Number:
Cite this article
Hua Han-bing, Bi Zheng-gang. Evaluation for fracture risk in elderly patients after hemiarthroplasty[J]. Chinese Journal of Tissue Engineering Research, 2014, 18(31): 5062-5067.
share this article
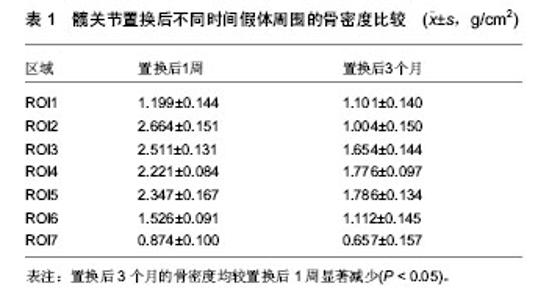
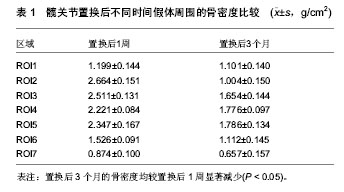
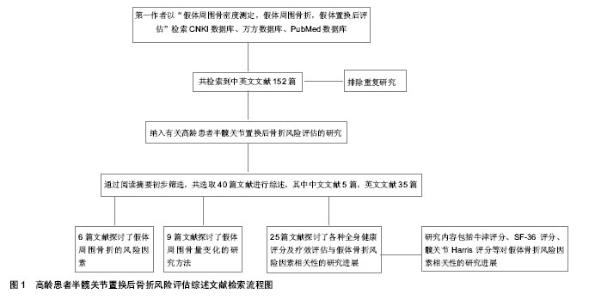
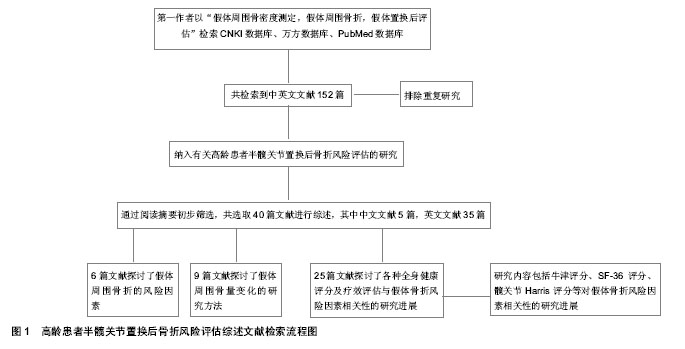
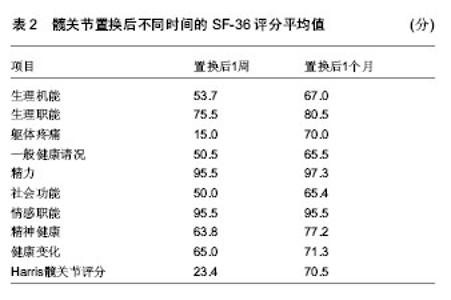
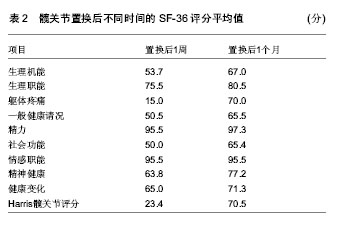
2.1 风险因素 2.1.1 组织学因素 自从半髋关节置换开展以来,学者们就坚持通过随访对置换后患者的并发症及风险因素各个方面进行评估和分析,其中包括南京医科大学范卫民等[2]的动物实验,在国内较早的证实了人工关节磨损后,产生大量的磨损微粒,微粒刺激组织细胞分泌肿瘤坏死因子等溶骨性因子,这些溶骨性因子直接或间接地激活破骨细胞,从而引起假体周围骨吸收、骨溶解,最终导致假体松动。假体松动后又可加重磨损,产生更多的微粒,形成恶性循环。 2.1.2 术中因素 刘志宏等[3]学者对人工髋关节置换后失败的病例进行分析,对人工髋关节翻修手术35例 (36髋)总结经验,根据前次手术失败的原因进行分组并分析。结果根据病例统计,在同一失败病例中,失败的原因往往不止一个。最常见的原因是假体松动、假体周围骨溶解,并得出结论,人工髋关节置换作为髋关节重建的一种有效的治疗方法而得到广泛的应用,其长期可靠的疗效与严格掌握手术指征,假体的适当选择和手术中正确操作有关。 2.1.3 自身因素 Burghardt等[4]曾通过HR-pQCT成像,证实2型糖尿病的高龄患者由于骨量重新分配的效率减慢,致使以牺牲皮质骨小梁的骨密度为代价来适应骨骼所受的弯曲外力。Singh等[5]对置换后患者平均6.3年的随访,认为对性别、疾病和肥胖的风险因素采取有效的干预措施针和优化疾病管理可以减少术后骨折的发生率。因此综合性指标的调查和研究,对于高龄患者将更为科学。 2.2 评价指标 2.2.1 双能X射线 双能X射线的临床应用使抽象的经验总结和动物实验对于临床工作中假体周围骨折的风险评估具体化,后在国内有学者临床放射学研究发现,股骨头假体置换后股骨周围常有骨质吸收现象并采用双能X射线骨密度测定及常规X射线检查对照方法,对12例股骨头置换患者术前、后假体周围骨量进行连续测定,认为双能X射线骨密度仪测定可作为人工股骨头或全髋置换后股骨假体松动的早期辅助诊断工具[6]。骨密度测定采用双能X射线骨密度仪并采用配套骨科分析软件进行分析按照Grune分7个测量兴趣区(region of interest,ROI)即将股骨柄假体从转子部到假体远端平均分为3等份,假体外侧从上到下分别为1区(ROI 1)、2区(ROI 2)、3 区(ROI 3),假体远端2 cm区域为 4 区(ROI 4),假体内侧从下到上分别为5区(ROI 5)、6区(ROI 6)和7区(ROI 7)。骨密度扫描时患者仰卧扫描床上,将膝及足固定标在标准位置以保持术肢内旋12°扫描时要避免因下肢旋转角度不良而致图像复制偏差。至今,通过使用双能X射线对髋关节置换后的患者进行假体周围骨密度动态观察[7-11],已经成为一种重要的研究手段,随后在研究中加入了Harris评分等术后疗效观察指标,使患者治疗效果的随访评估更加完善。 2.2.2 疗效评分系统 牛津髋关节评分系统:与以往的其他的人工髋关节置换评价体系不同,该评分系统属于医疗处置结果评估体系,是基于患者本人感觉的量表,该评价系统的可靠性和敏感性已被证实,问题简单易懂,适用于各种文化程度的患者,尤其是能以信件,电话的方式进行询问。特点是短小,灵活,方便,具有临床使用价值。 采用世界卫生组织(WHO)推荐的“健康调查简易量表”(SF-36):该量表由36个单项组成,包括8个维度,均按百分制进行评分:①体能。②精神影响。③社会活动。④心理健康。⑤体能影响。⑥精力。⑦身体疼痛。⑧一般健康。各维度计分采用累加法,按最后题值计算原始分数,再以标准公式计算转换分数,各维度得分为0分(最差)-100分(最好)[12]。日本有学者使用SF-36评分对肢体功能障碍术后患者的全身健康状态进行评估,证实了该评估手段与骨折风险的相关性。Baker等[13]在人身体质量指数对假体置换后功能性改进的实验中,通过体质量指数所反应的效应与SF-36所显示的一致。 目测类比评分法:该法比较灵敏,有可比性。具体做法是:在纸上面划一条10 cm的横线,横线的一端为0,表示无痛;另一端为10,表示剧痛;中间部分表示不同程度的疼痛。让患者根据自我感觉在横线上划一记号,表示疼痛的程度。轻度疼痛平均值为2.57±1.04;中度疼痛平均值为5.18±1.41;重度疼痛平均值为8.41±1.35。测定可分别在假体置换后1周、3个月、6个月、1年时进行。因此综合全面量化统计将会成为评估未来髋关节置换后骨折风险的一个大体趋势,尤其是试用于高龄患者[14-15]。 自行共病调查问卷(SCQ):诸如Sangha等[16]所倡导的自行共病调查问卷和心理评估等等也可用于置换后患者的综合评估范围之内。Anderson等[17]在评价患者年龄在75岁以上全膝关节置换后功能结果和患者满意度时所采用的疗效评价方法,虽然只做了回顾性的分析但相对全面。其结论明确显示了,心理评估分数与患者置换后功能情况有明显的相关性。 Harris人工髋关节疗效评分:包括疼痛、功能性活动、髋关节活动度及畸形4 个组成部分。其中,疼痛和功能性活动在Harris评分法中比重较大[18],两部分共计62分,因此无需再用日常生活能力评估量表(ADL)或功能独立性测量(FlM)等评估工具重复评定[4]。Harris 评分法在国内外髋关节置换疗效评价中都得到了一定的应用,国内有不少的髋关节置换疗效文献都使用了Harris评分法[19]。2.3 现状分析 Ethgen等[20]用Medline和EMBASE医疗文献数据库搜索,从1980年1月到2003年6月,识别相关的研究。研究资格审查是否符合以下标准:①语言是英语或法语。②至少一个有效的和自我报告健康相关生活质量的仪器。③一个前瞻性群组研究或设计使用。认为健康相关生活质量的数据是有价值的。而近年来,随着双能X射线的发展和普及,辐射小,价格低廉,成为研究骨量变化的重要检测手段[21],例如Singh[22]和Korkosz等[23]对强直性脊柱炎患者骨密度的测定过程中,显著肯定了双能X射线吸收仪的优势。 2.3.1 临床资料 哈尔滨医科大学附属第一医院2013年8月至12月对7例髋关节置换后的患者进行随访时获得数据,假体周围骨折的患者在翻修入院后测定。应用双能X射线骨密度仪等检查设备观察此后1年髋关节置换后的患者假体周围的骨密度。男6例,女1例,70-74岁,平均73岁,右髋4例,左髋3例,其中股骨头骨折患者6例,股骨头坏死1例,所有患者均无长期应用激素的病史,并排除所有其他代谢性骨病。所有患者均行髋关节置换,采用生物型髋关节假体,康复方法大致相同。分别于置换后1周、3个月、6个月、12个月行假体周围骨密度等指标的测定。 2.3.2 骨密度测量 采用美国数字式双能X射线骨密度仪,及其附带的骨科分析软件,所有测量及分析工作均由同1人完成。对膝关节假体周围骨质进行分区测定。 2.3.3 骨密度扫描变异系数 按Callaghan的方法计算变异系数[24],连续2 d测量5例患者的骨密度,每天测定1次,计算所测各个兴趣区的变异系数。ROI1-7区的CV%为(0.6±0.11)%。 2.3.4 统计学处理 分别将术后3,6,12个月时的骨密度检测值与术后1周时的骨密度检测值进行比较,采用单因素方差分析[25],并计算术后3,6,12 个月时骨密度(骨密度)变化率。骨密度变化率= [(骨密度2-骨密度1)÷骨密度1]×100% 骨密度1为术后1周时的骨密度值;骨密度2为3,6,12个月时的骨密度值[26]。 2.3.5 结果 所有患者均于1 周内完全负重,并暂时得到了3个月随访,术后无感染和假体松动现象,功能恢复良好。 置换后假体周围骨密度测定结果:表1可见置换后3个月的骨密度均较置换后1周显著减少(P < 0.05)。 置换后功能评分结果:表2可见置换后1个月的SF-36评分较置换后1周显著升高(P < 0.05)[27-30]。"
"
"
| [1] Kynaston-Pearson F, Ashmore AM, Malak TT, et al. Primary hip replacement prostheses and their evidence base: systematic review of literature. BMJ. 2013;347:f6956. [2] 范卫民,王青,陶松年,等.人工关节松动病因的研究[J].中华骨科杂志,1998,18(9):518-521. [3] 刘志宏,王毅,杨庆铭,等.人工髋关节置换术失败原因分析[J].中华骨科杂志,2000,20(12):723-727. [4] Burghardt AJ, Issever AS, Schwartz AV, et al. High-resolution peripheral quantitative computed tomographic imaging of cortical and trabecular bone microarchitecture in patients with type 2 diabetes mellitus. J Clin Endocrinol Metab. 2010;95: 5045-5055. [5] Singh JA, Jensen MR, Harmsen SW, et al. Are gender, comorbidity, and obesity risk factors for postoperative periprosthetic fractures after primary total hip arthroplasty? J Arthroplasty. 2013;28(1):126-131.e1-2. [6] Napoli N, Schwartz AV, Palermo L, et al. Risk factors for subtrochanteric and diaphyseal fractures: the study of osteoporotic fractures. J Clin Endocrinol Metab. 2013;98(2): 659-667. [7] Rizzoli R, Akesson K, Bouxsein M, et al. Subtrochanteric fractures after long-term treatment with bisphosphonates: a European Society on Clinical and Economic Aspects of Osteoporosis and Osteoarthritis, and International Osteoporosis Foundation Working Group Report. Osteoporos Int. 2011;22:373-390. [8] 林剑浩,吕厚山,寇伯龙,等.股骨头假体置换术后假体周围骨量变化的观察[J].中华骨科杂志,1995 ,15(8):494-499. [9] Melton 3rd LJ, Riggs BL, Leibson CL, et al. A bone structural basis for fracture risk in diabetes. J Clin Endocrinol Metab. 2008;93:4804-4809. [10] Palazzo C, Jourdan C, Descamps S, et al. Determinants of satisfaction 1 year after total hip arthroplasty: the role of expectations fulfilment. BMC Musculoskelet Disord. 2014; 15:53. [11] 王文昊.人工全髋关节置换术失败原因及翻修术的疗效观察[D]. 山东大学,2013. [12] Callaghan JJ, Dysart HD, Savory CF, et al. Assessing theresults of hip replacement. Bone Joint Surg Br. 1990; 72(10): 1008- 1009. [13] Baker P, Muthumayandi K, Gerrand C, et al. Influence of body mass index (BMI) on functional improvements at 3 years following total knee replacement: a retrospective cohort study. PLoS One. 2013;8(3):e59079. [14] Li MG, Nilsson KG. Changes in bone mineral density at theproximal tibia after total knee arthroplasty: a 2- year followupof 28 knees using dual energy X- ray absorptiometry.J Orthop Res. 2000;18(1): 40-47. [15] Karachalios T, Tsatsaronis C, Efraimis G, et al. The long- term clinical relevance of calcar atrophy caused by stress shielding in total hip arthroplasty: a 10-year, prospective, randomized study. J Arthroplasty. 2004;19: 469-475. [16] Sangha O, Stucki G, Liang MH, et al. The Self-Administered Comorbidity Questionnaire: a new method to assess comorbidity for clinical and health services research. Arthritis Rheum. 2003;49(2): 156-163. [17] Anderson JG, Wilson RL, Tsai D, et al. Functional outcome and patient satisfaction in total knee patients over the age of 75. J Arthroplasty. 1996;11(7): 831-840. [18] 沈霖, Sabo D, Ewerbeck V. 全髋关节置换术后假体周围骨密度动态观察[J].中国中医骨伤科杂志, 2001,9(3):1-4. [19] World Health Organisation BMI classification. 2012. [20] Ethgen O, Bruyère O, Richy F, et al. Health-related quality of life in total hip and total knee arthroplasty. A qualitative and systematic review of the literature. J Bone Joint Surg Am. 2004;86-A(5):963-974. [21] Jones CA, Voaklander DC, Johnston DW, et al. Health related quality of life outcomes after total hip and knee arthroplasties in a community based population. J Rheumatol. 2000;27(7): 1745-1752. [22] Singh HJ, Nimarpreet K, Ashima Das S, et al. Study of bone mineral density in patients with ankylosing spondylitis. J Clin Diagn Res. 2013;7(12):2832-2835. [23] Korkosz M , G?sowski J , Grzanka P ,et al. Baseline new bone formation does not predict bone loss in ankylosing spondylitis as assessed by quantitative computed tomography (QCT): 10-year follow-up. BMC Musculoskelet Disord. 2011;12:121. [24] Moritomo H , Imaeda T , Gotani H , et al. Reliability of the hand20 questionnaire: comparison with the 36-item short-form health survey. Hand Surg. 2014;19(1):1-6. [25] Bruyère O , Ethgen O , Neuprez A , et al. Health-related quality of life after total knee or hip replacement for osteoarthritis: a 7-year prospective study. Arch Orthop Trauma Surg. 2012;132(11):1583-1587. [26] Chiu HC, Mau LW, Hsu YC, et al. Postoperative 6-month and 1-year evaluation of health-related quality of life in total hipreplacement patients. J Formos Med Associ. 2001; 100(7): 461-465. [27] Towheed TE, Hochberg MC. Health-related quality of life after total hip replacement. Semin Arthritis Rheum. 1996; 26(1): 483-491. [28] Cleary PD, Reilly DT, Greenfield S, et al. Using patient reports to assess health-related quality of life after total hip replacement. Qual Life Res. 1993; 2(1):3-11. [29] Shi HY , Chiu HC , Chang JK , et al. Evaluation and prediction of health-related quality of life for total hip replacement among Chinese in Taiwan. Int Orthop. 2008; 32(1):27-32. [30] Uesugi Y, Makimoto K, Fujita K, et al. Validity and responsiveness of the Oxford hip score in a prospective study with Japanese total hiparthroplasty patients. J Orthop Sci. 2009; 14(1):35-39. [31] Badura-Brzoza K, Zajac P, Brzoza Z, et al. Psychological and psychiatric factors related to health-related quality of life after total hip replacement - preliminary report. Eur Psychiatry. 2009;24(2):119-124. [32] Shi HY, Khan M, Culbertson R, et al. Health-related quality of life after total hip replacement: a Taiwan study. Int Orthop. 2009; 33(5):1217-1222. [33] Santi? V, Legovi? D, Sestan B, et al. Measuring improvement following total hip and knee arthroplasty using the SF-36 Health Survey. Coll Antropol. 2012;36(1):207-212. [34] Hofhuis JG , Spronk PE. Health-related quality of life and influence of age after trauma: An overview. J Trauma Acute Care Surg. 2014;76(2):549-556. [35] Guillemin F, Martinez L, Calvert M, et al. Fear of falling, fracture history, and comorbidities are associated with health-related quality of lifeamong European and US women with osteoporosis in a large international study. Osteoporos Int. 2013;24(12):3001-3010. [36] Liu SS, Buvanendran A, Rathmell JP, et al. A cross-sectional survey on prevalence and risk factors for persistent postsurgical pain 1 year after total hip and knee replacement. Reg Anesth Pain Med. 2012;37(4):415-422. [37] Stevens M, Paans N, Wagenmakers R, et al. The influence of overweight/obesity on patient-perceived physical functioning and health-relatedquality of life after primary total hip arthroplasty. Obes Surg. 2012;22(4):523-529. [38] Bolton KL, Egerton T, Wark J, et al. Effects of exercise on bone density and falls risk factors in post-menopausal women with osteopenia: a randomised controlled trial. J Sci Med Sport. 2012;15(2):102-109. [39] Garrido-Abejar M, Serrano-Parra MD, Bartolomé-Gutiérrez R, et al. [Factors associated with health-related quality of life in the institutionalised elderly: differences between men and women]. Enferm Clín. 2012;22(1):27-34. [40] Vlak T, Kaštelan D, Lozo P,et al. Monthly or weekly bisphosphonate? Evaluation of satisfaction in patients with postmenopausal osteoporosis using OPSAT-Q questionnaire during the BOOSTER study in Croatia. Clin Rheumatol. 2011; 30 (12):1549-1554. |
| [1] | Fang Yi, Zhao Wenzhi, Pan Deyue, Han Xin, Zhang Lu, He Hongtao, Shi Feng, Tian Tingxiao. Acromioclavicular joint dislocation: how to achieve anatomical reduction, sustained stability and micro-motion [J]. Chinese Journal of Tissue Engineering Research, 2020, 24(5): 796-802. |
| [2] | Fu Jiaxin, Xiao Lianping, Wang Shusen, Li Xiaodong, Han Liqiang, Wang Tonghao. Therapeutic effects of paraspinal approach combined with internal fixation through pedicle of fractured vertebra versus traditional AF screw-rod system for thoracolumbar fractures [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(8): 1177-1181. |
| [3] | Qiu Zhongpeng, Li Ke, Li Gang, Liu Keyu, Du Xinhui, Meng Defeng, Shi Chenhui, Wang Weishan. Different treatments for two-part and three-part proximal humeral fractures by Neer classification: follow-up results analyzed using clinical economics [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(8): 1188-1195. |
| [4] | Ke Wei, Li Ke, Wang Sibo, Du Xinhui, Qiu Zhongpeng, Kang Zhilin, Wang Weishan, Li Gang . Open reduction and plate fixation versus closed reduction and external fixation for distal radius fractures: scores and linear regression analysis [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(8): 1196-1202. |
| [5] | Fan Zhirong, Peng Jiajie, Zhong Degui, Zhou Lin, Su Haitao, Huang Yongquan, Wu Jianglin, Liang Yihao. Suture anchor combined with open reduction and internal fixation versus open reduction and internal fixation for ankle fracture combined with deltoid ligament injury: a meta-analysis [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(8): 1307-1312. |
| [6] | Zhou Yu, Liu Yuehong, Liu Shuping, Chen Xi, Qin Wei, Li Qifeng. Spinal stability of intervertebral grafting reinforced by five or six augmenting screws versus transvertebral grafting reinforced by four augmenting screws for thoracolumbar vertebral fractures [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(4): 505-511. |
| [7] | Li Xianzhou, Wang Qian, Zhang Cunxin . Lumbar spondylolisthesis: status and prospects of implant treatment [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(4): 621-627. |
| [8] | Yin Hao, Zhou Enchang, Pan Zhengjun, Chen Guang, Jiang Hua. Finite element analysis of the four and three cannulated screws combined with buttress plate fixation for the treatment of Pauwels III femoral neck fractures [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(32): 5133-5137. |
| [9] |
Wang Lei, Li Zilong, Yuan Binbin, Wu Qingwei, Tang Fengming.
Clinical effect of locking plate versus anterograde intramedullary nail in the treatment of adult humeral shaft fractures: a meta-analysis
[J]. Chinese Journal of Tissue Engineering Research, 2019, 23(24): 3924-3930.
|
| [10] | Hao Liang, Zhang Zhonglin, Wang Baodong, Bi Zhenggang. Intertrochanteric fracture of the femur: improvement of internal fixation device, surgical changes and related disputes [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(18): 2927-2935. |
| [11] | Yao Liquan, Ling Qinjie, Li Jiaying, Zhong Letian, Zhou Xingping, Liu Jintao, He Erxing, Yin Zhixun. Antibiotic artificial bone implantation for treating pyogenic spondylodiscitis [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(14): 2133-2139. |
| [12] | Gong Zhibing, Wu Zhaoke, Zhang Huantang, Xu Zhiqing, Zhuang Zhikun, Zhang Qianjin. Allogeneic cortical bone plate combined with locking plate for Vancouver type B1 and C osteoporotic periprosthetic femoral fractures after hip arthroplasty in older adults [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(12): 1812-1817. |
| [13] | Li Xiaofeng, Xie Furong, Zhan Long, Yang Yuan. Design of locking compression plate through transoral approach [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(12): 1824-1828. |
| [14] | Tian Youyong, Wang Zhiyong. Short-term follow-up of dynamic hip screw versus proximal femoral nail anti-rotation for type AO/OTA A1 intertrochanteric femoral fracture in older adults [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(12): 1834-1839. |
| [15] | Huang Weiyan, Peng Jiewei, Wan Ming, Zheng Xiaoming, Wang Kangzhen. Four internal fixation methods of proximal femoral nail, locking compression plate, dynamic hip screw, and Gamma nail for treating senile intertrochanteric fractures [J]. Chinese Journal of Tissue Engineering Research, 2019, 23(12): 1846-1852. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||